Resources & Social Support for Brain Injury Survivors
The Skinny on Splints
DISCLAIMER: Please follow the direction of your treating physician, physical therapist, or occupational therapist. This information should be used to augment rather than replace skilled intervention or professional advice.
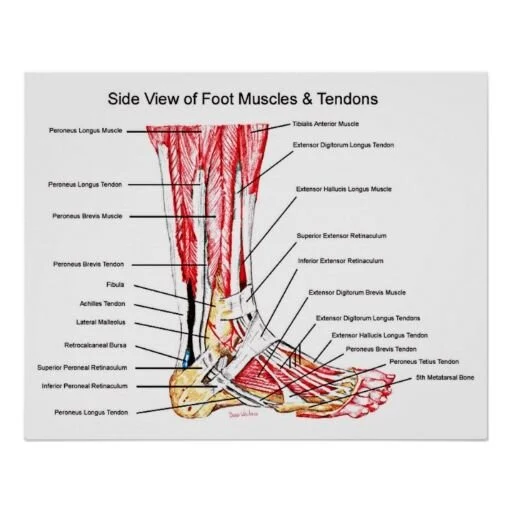
An Ankle Foot Orthosis (AFO) is a great tool for foot drop. In those first several of weeks of recovery an AFO allows survivors to walk when they have no control of their ankle, shin, and calf. It allows the survivor to work on the bigger muscles of their hips and thighs in order to walk. For many people post-brain injury, it is an essential part of their treatment plan.
Here is my beef with the AFO: They are effective at the beginning of treatment and when you have no functional movement. However, as you progress, an AFO can become a splint that shortens your muscles and tendons, thereby making it difficult to perform the crucial movement required to lift your foot. My whole body cringes when people begin to work on sit-to-stand with their AFO on even early on in their recovery. If you are not walking, this is a perfect opportunity to stretch the tendons of your ankle, practice shifting your weight and using your tibia to shift, and lift your toes while flexing your ankle upward.
There are a lot of benefits to weight-bearing through your foot sans your AFO, socks, and shoes. With your AFO on, your foot is getting some weight-bearing, but it is not significant. In this scenario, it is much easier to compensate by leaning on your less affected leg with an AFO visually and physically cueing your brain not to put full weight on it. When you do put weight on your AFO strapped foot, your tibia never gets that full feeling of weight so the joints of your knee and ankle do not get as sensitive information. Keeping your ankle and your knee in one place is not normal movement. Joints normally glide and move at angles, however with an AFO your joint can only move in one or two directions. It’s like using WWII sonar information instead of radar to find your way through space.
Here is the gist: Yes, we want you to wear your AFO when walking, especially long distances, but when you are doing sit-to-stands it is important to let your leg and foot breathe. This allows your joints to articulate and your brain to get a full map of where your foot is in space. If you have spasticity in that ankle and foot, that is NOT a reason to keep the AFO on. On the contrary, getting your foot out and letting your toes feel the pressure of your weight will decrease curling and discomfort.
The moral of the story is to use your AFO when you need it for walking, but then practice without it. You’re future self will thank you.
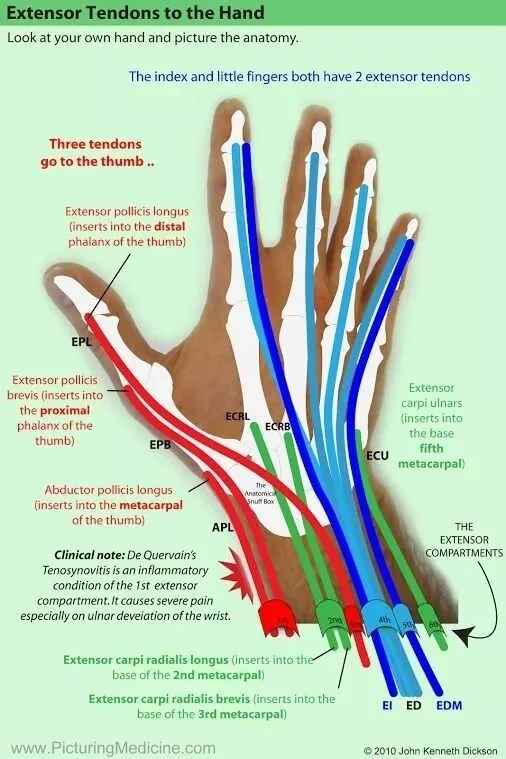
Now, for the hand, this is where I lose my mind. Often, what happens is that survivors keep using their AFO forever and discontinue using their resting night splint because it is mildly uncomfortable or because nobody explained its purpose. This makes me feel insane. If you have a spastic or flaccid hand, you need a resting night splint. It is important to wear this splint every single night. NO exceptions, unless your hand is completely unaffected. If you have absolutely no issues, then by all means discontinue your splint, but for everyone else: ear the damn thing.
Here is why: reflexes and spasticity are very closely linked. Ever noticed how your hand opens or closes when you are yawning or sneezing? There is a connection there. When you sleep, you are unaware of the reflexes happening and your hand responds to your relaxed state often with increased spasticity. If this is happening while you sleep then your brain and hand are getting eight to ten hours of training in the wrong direction. Instead of waking up with a slighly sore wrist and fingers, you wake up with a fisted hand. It is so much easier than an AFO. Occasionally it is uncomfortable, but it can be adjusted for comfort and it is ten hours of practice where you don’t have to do anything. It is a no brainer!
Moreover, if you have a flaccid hand or a hand that does not have any volitional movement, then you need this splint to set your wrist. With a low tone or atrophied wrist and forearm, the wrist tends to droop into flexion. Normal for the wrist is neutral; where the wrist is neither up or down. Normal can also be a teensy bit up in the direction of a wave, but it is never down. What happens here is that the hand does not have the normal protective tone, movement, or position sense to protect the ligaments, bones, and tissue of the hand from injury when you are unconsciously dozing. When the wrist is kept in a flexed position, one of the tiny bones in the wrist called the scaphoid often moves up the wrist out of place making it doubly difficult to raise your wrist in an extension pattern.
Moral of the story: wear your resting night splint. Do not stop until a medical practitioner is absolutely certain you do not need it any longer. Your future self will thank you.